|
|
Otorhinolaryngology Otorhinolaryngology |
|
|
")
|

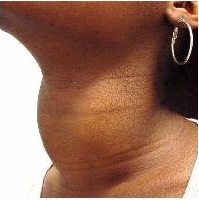
Neck Lump
The etiology of neck lumps are numerous and present a good opportunity to cover the "surgical sieve"
The surgical sieve allows you to answer a "what are the causes of..." question (whether on ward rounds or exams) in a systematic way. Using the VITAMIN CD acronym, for neck lumps it can be constructed like this:
Vascular: AV malformation, aneurysm
Inflammatory: Submandibular sialadenitis
Traumatic: Ranula, haematoma
Autoimmune/allergic: Thyroiditis
Metabolic: Goitre
Infective: Lymphadenitis, reactive lymphadenopathy, TB
Neoplastic
Benign: Carotid body tumour/chemodectoma
Malignant: Metastatic squamous cell carcinoma, thyroid cancer, lymphoma
Congenital: Branchial cyst, thyroglossal duct cyst, dermoid cyst
Degenerative
If you'd like to read more about surgical sieves see http://en.wikipedia.org/wiki/Surgical_sieve
Now more about neck lumps...
|
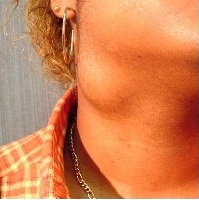
Branchial cleft cyst |
Goitre |
Thyroglossal duct cyst |
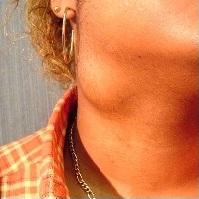

Click on the images to get a description

History
Important points to cover when taking a neck lump history:
- Pain: chronic oral pain is suspicious of malignancy and referred unilateral otalgia can be associated with tumours at the base of the tongue, larynx and laryngopharynx (due to CN IX and X innervating both the pharynx and the ear)
- Dysphagia: range of occasional "catching" to inability of swallowing solids. Tumours generally cause gradual decline in ability to swallow food and weight loss. Nasal regurgitation or aspiration suggests neurological cause.
- Stridor: inspiratory sounds - caused by airflow blockage at or above the vocal cords i.e. is a symptom of upper respiratory obstruction.
- Hoarseness: suggests laryngeal disease - needs referral to ENT
- Constitutional symptoms: weight loss, night sweats, anorexia, chills/fevers - suggestive of malignancy
- Social factors: smoking and alcohol - highly associated with head and neck cancers. HPV from sexual partners is fast overtaking smoking as a risk factor
|
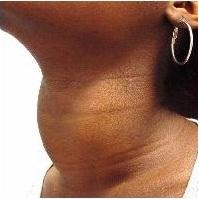
Pre-operative photo |
Intra-operative photo |
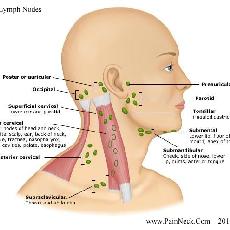
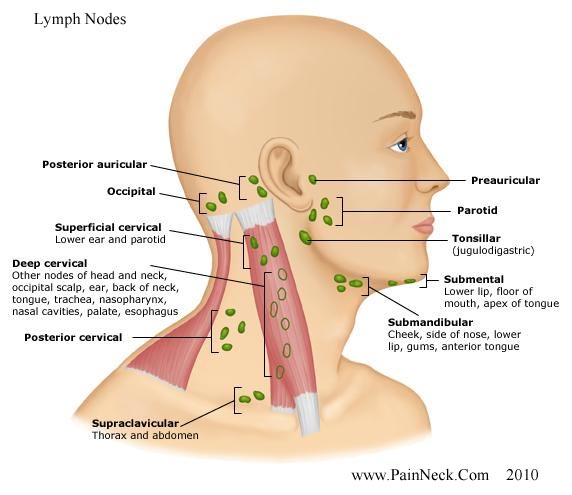
Cervical lymph nodes |




Examination
Requires a full ENT examination as cancer can hide in a lot of places! A full ENT examination includes:
1. A thorough neck examination including the thyroid, lymph nodes, parotid & submandibular glands - Note: the neck is examined from behind the patient after initial inspection
Lumps should be assessed for:
Position
Size
Contour - smooth, craggy
Texture - soft, firm, hard or fluctuant
Mobility
Tenderness
2. Examination of the ears
3. Anterior rhinoscopy - using a headlight and thudicum speculum
4. Oral cavity examination
5. Cranial nerve exam
6. Flexible nasendoscopy
7. Skin of the head and neck - looking for malignant lesions - especially important in New Zealand and Australia
8. Look for signs of hypo- or hyper- thyroidism
Please watch the videos at the start of each section as they highlight examination techniques and findings
Investigations
1. Imaging: Ultrasound, CT or MRI
2. Cytology/histology: Fine needle aspiration (FNA) or biopsy
3. Blood tests
FBC - useful if haematological condition suspected
Thyroid function tests - useful in thyroid disease
After the above: ENT specialists, in conjunction with other specialties, may order tertiary investigations such as PET-CT and carry out tertiary invasive investigations such as panendoscopy. However, this is beyond medical school curricula
|
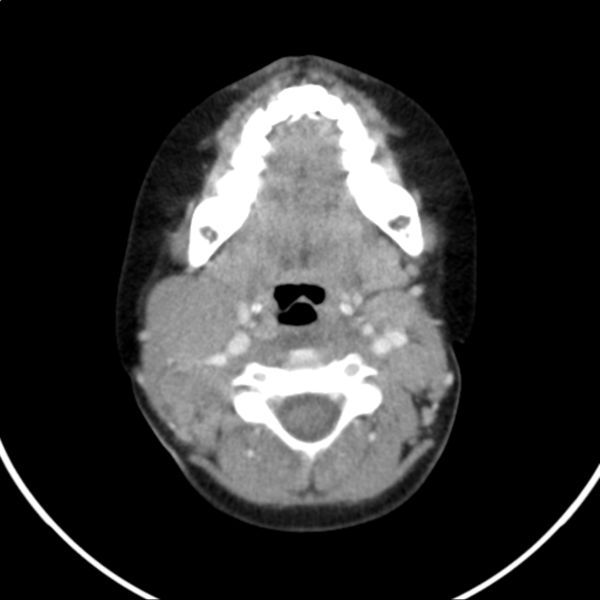
The CT on the right is of a patient who presented with a neck lump and weight loss over 6 months. On examination the patient had a large neck mass at the right angle of the jaw. It was firm, smooth, minimally mobile and non-tender. The patient also had lymphadenopathy in the left cervical chain, left and right axillae.
The CT shows a ~4cm mass in the area of the jugulodigastric lymph node. The CT along with the history and examination is suggestive of a lymphoma. |