|
|
Otorhinolaryngology Otorhinolaryngology |
|
|
")
|

Deep Neck Space Infections
The anatomy of the neck is complex. To understand the origin and spread of deep neck space infections (DNSI) a basic understanding of the anatomy is required
Summary of anatomical concepts:
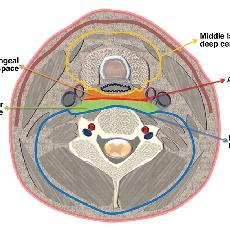
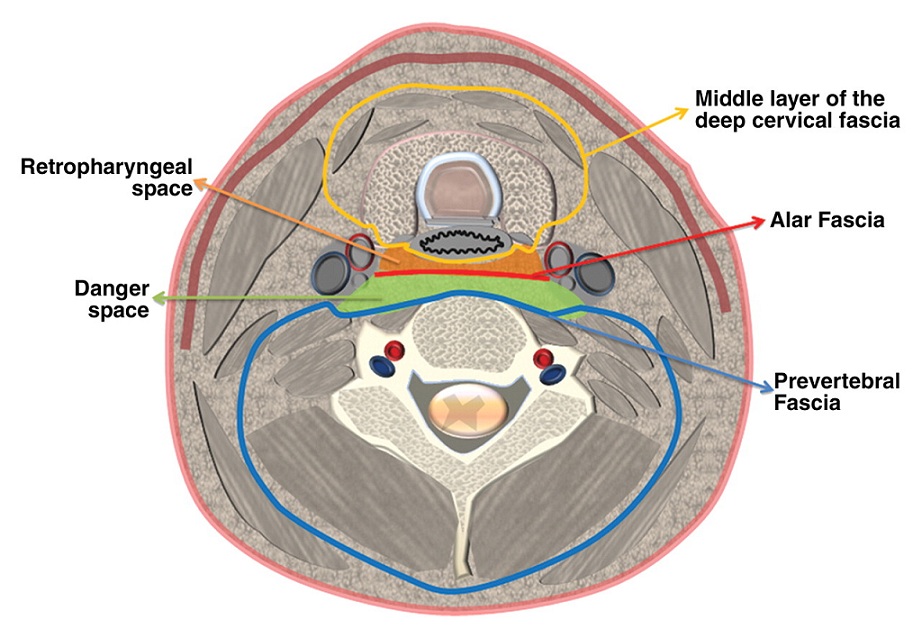
- Spatial compartments in the neck are created by fascial planes
- These spatial compartments can communicate with each other -> spread of infection
- Anterior to the prevertebral fascia is the dramatically named "danger space" that extends from the skull base to the diaphragm - meaning mediastinitis is a possible complication of abscesses that spread into this space
- There are a number of important structures in this area including blood vessels, nerves & bone that can become affected
Types of DNSI:
1. PTA/quinsy (see previous page)
2. Retropharyngeal abscess
3. Parapharyngeal abscess
4. Prevertebral abscess
5. Submandibular abscess (relatively superficial)
Challenge to diagnosis: DNSI may be covered by layers of unaffected tissues & therefore can be hard to visualise and palpate
|
Neck fascial planes anatomy |
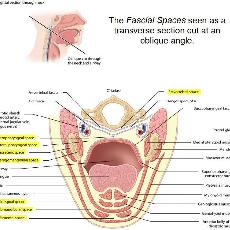
Neck anatomy |
Etiology
DNSI are most commonly complications of pharyngitis or dental infection
Other causes include: sialadenitis, IV drug use, malignancy
Note: DNSI is often a complication of an inadequately treated pharyngitis, dental abscess or tonsillitis
Important possible sequela of DNSI:
Carotid artery rupture, meningitis and cavernous sinus thromboses are rare
- Internal jugular vein thrombophlebitis (Lemierre Syndrome) - can cause septic emboli and sepsis
- Mediastinitis - signalled by chest pain or widened mediastinum on CXR
|
CXR - widened mediastinum |
CT Mediastinitis |


- Sore throat, dysphagia, odynophagia, trismus
- Neck pain and pain on neck movement
- Can have painful neck mass
- Posterior pharynx erythema + swelling in retropharyngeal abscess
- Medial displacement of tonsil and lateral pharyngeal wall in parapharyngeal abscess
- Torticollis (holds neck in rotated position)
- Tender lymphadenopathy
Findings suggesting complications:
- Neurological deficit - cranial nerves (eg. hoarseness from vocal cord paralysis with carotid sheath and X/recurrent laryngeal nerve involvement)
- Horner syndrome from involvement of the cervical sympathetic chain
Investigations
1. CT neck
2. FBC, U+E
3. Blood cultures


Lateral neck X-ray on left showing prevertebral soft tissue thickening
The CT scan on the right shows extent of abscess
.
.
.
.
.
.
Management
1. ABC's
As with PTA/Quinsy the airway is of paramount importance
Followed by IV fluid resus for the "C"
2. Antibiotics
3. Surgery - incision and drainage

 This young boy presented with a history of having had a sore throat. Over some days he developed worsening fevers, trismus and this fluctuant swelling in his left submandibular region (left picture)
This young boy presented with a history of having had a sore throat. Over some days he developed worsening fevers, trismus and this fluctuant swelling in his left submandibular region (left picture)
Diagnosis = submandibular abscess and it was treated with incision and drainage (right picture)
.
Note: Submandibular abscesses, like the one in the picture above, are the most superficial of the DNSI. They occur most commonly secondary to dental infections or peritonsillar cellulitis. Retropharyngeal and parapharyngeal abscesses are not as easily seen externally.
| « Sore throat | Neck Lump » |

