|
|
Otorhinolaryngology Otorhinolaryngology |
|
|
")
|

Hoarseness or Voice Change
Voice change or dysphonia (including hoarseness) is a symptom of primary laryngeal disease although rarely it can be due to other diseases e.g. lung cancer or hypothyroidism
The function of the larynx is primarily phonation and airway protection
The normal larynx:
1. Vocal fold (cord)
2. Vestibular ligament/fold
3. Epiglottis
4. Aryepiglottic fold
5. Corniculate cartilage
6. Piriform sinus
7. Lingual tonsil
Etiology
Every patient that presents with dysphonia needs to have malignancy excluded
The common causes of dysphonia are (remember the surgical sieve):
Trauma - phonotrauma - voice abuse & misuse leads to trauma of the vocal cords. Repetitive phonotrauma leads to a local inflammatory response which can progress to nodules and polyps
Neoplasm
Benign lesions (not neoplasms but are "growths"): Vocal fold nodule, vocal fold polyp, vocal fold papilloma, laryngeal cysts
Malignant neoplasms: Laryngeal SCC (>90% of laryngeal cancer)
Multiple underlying pathological mechanisms: vocal cord paralysis or recurrent laryngeal nerve paralysis
|
Recurrent respiratory papillomatosis |
Vocal fold polyp |
Vocal fold cyst |
Vocal fold nodule |
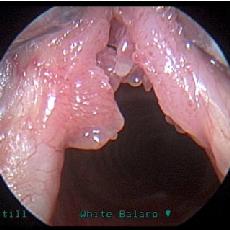
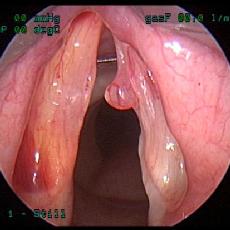
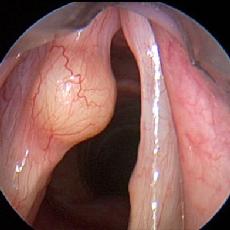
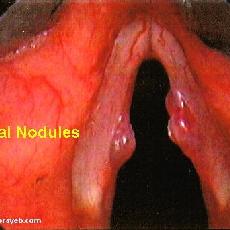
Benign laryngeal neoplasms (click image to enlarge)



History
- The onset, duration and progression of any voice change
- Preceding upper respiratory tract infections, direct or vocal trauma and endotracheal intubation
- Social factors: particularly smoking and alcohol
Occupation - professional voice users have higher rates of benign laryngeal disease as they have higher rates of voice misuse and abuse - therefore a careful history of voice use is needed - Systemic enquiry should include symptoms of hypothyroidism and gastro-oesophageal reflux disease (GORD)
Age is very important:
- Adults have a greater incidence of malignant disease
- In children the main differential diagnosis is vocal cord nodules and laryngeal papillomatosis
Persistent and progressive dysphonia in a person with a smoking history is a red flag for laryngeal malignancy - especially if associated with dysphagia or odynophagia
Examination
1. A full ENT exam (see Head and Neck section) with a focus on a flexible nasendoscopic examination of the larynx
2. Video stroboscopy - allows visualisation of the mucosal wave and has an appearance of a "slow motion" film. It is useful in diagnosis, monitoring rehabilitation and speech therapy
 .
.
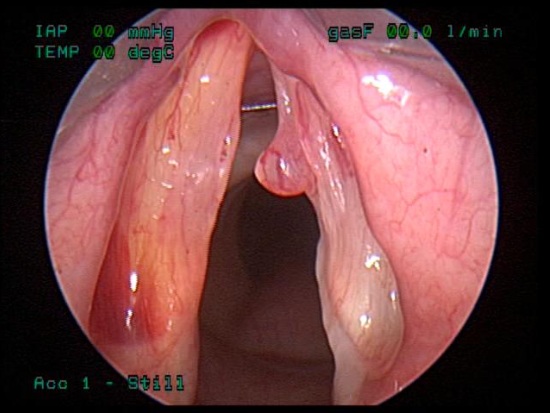
Compare this picture with the pictures above. What are the main differences?
.
.
.
.
You may have chosen to comment on:
- "yuck factor" - cancers generally are craggy, asymmetrical and show signs of active inflammation
- it appears to be invading surrounding structures rather than "pushing" them to the side
- it is larger than the other lesions
Treatment of Laryngeal Cancer
Treatment strategy depends on histology type, grade, tumour stage and overall health of the patient
Like most major cancers, this requires an MDT approach involving:
- Surgeon
- Speech language therapist
- Specialist nurses e.g. tracheostomy nurse
- Dietician
- Radiologist
- Radiation oncologist
- Medical oncologist
- Pathologist
The mainstay of treatment involves:
- Surgery - partial or total laryngectomy (the latter requiring a tracheostomy)
+/- reconstruction using surgical flaps - Radiotherapy - primary or adjuvant
- Chemotherapy in some cases
|
Treatment of vocal fold papilloma Click on the picture on the right to watch the video First the video shows the patient coughing with papilloma evident on both vocal folds The surgeon then uses coblation (radiofrequency ablation) to remove the papilloma |
Transforming into HTML5 Videos/Audios, please check this page after 10 minutesCoblation of papilloma
|
Transforming into HTML5 Videos/Audios, please check this page after 10 minutesNasoendoscopy of a normal larynx. The patient is asked to whistle "Happy Birthday"
Note how the vocal cords move symmetrically The second half of the video shows stroboscopy (darkened), this allows you to better visualise vocal cord movement |
Transforming into HTML5 Videos/Audios, please check this page after 10 minutesNasoendoscopy of a person with a left sided recurrent larygneal nerve palsy
The patient is attempting to whistle Note how the vocal cords move unsymmetrically and do not come together The second half of the video shows stroboscopy (darkened), this allows you to better visualise vocal cord movement |

